A mammogram is a radiographic examination showing the morphology and structure of the anatomical elements of the breast tissue and any pathological lesions it may present. Today, three decades after the initial implementation of mammography in preventing breast cancer, it continues to be the method of choice for the early diagnosis of the disease.
A mammogram is one of the most important examinations in the framework of annual screening for women over the age of 40. The American College of Radiology recommends annual screening beginning at age 40 and this is what we recommend at Diagnostic Mammography. Women who are considered high risk may need to start mammography earlier. When a woman presents for her annual breast examination, without the presence of any clinical findings found by herself or by her doctor we refer to the examination as a “screening mammography”. At “Diagnostic Mammography”, our qualified personnel informs our women of the procedure of mammography technique and then proceeds to record a detailed personal and family history. When recording the woman’s history, emphasis is given to any prior surgical biopsies to allow the placement of identification skin markers. On the day of the examination it would be preferable for women to avoid using deodorant or talcum powder as their use may lead to an incorrect interpretation of the mammogram.
Diagnostic mammography
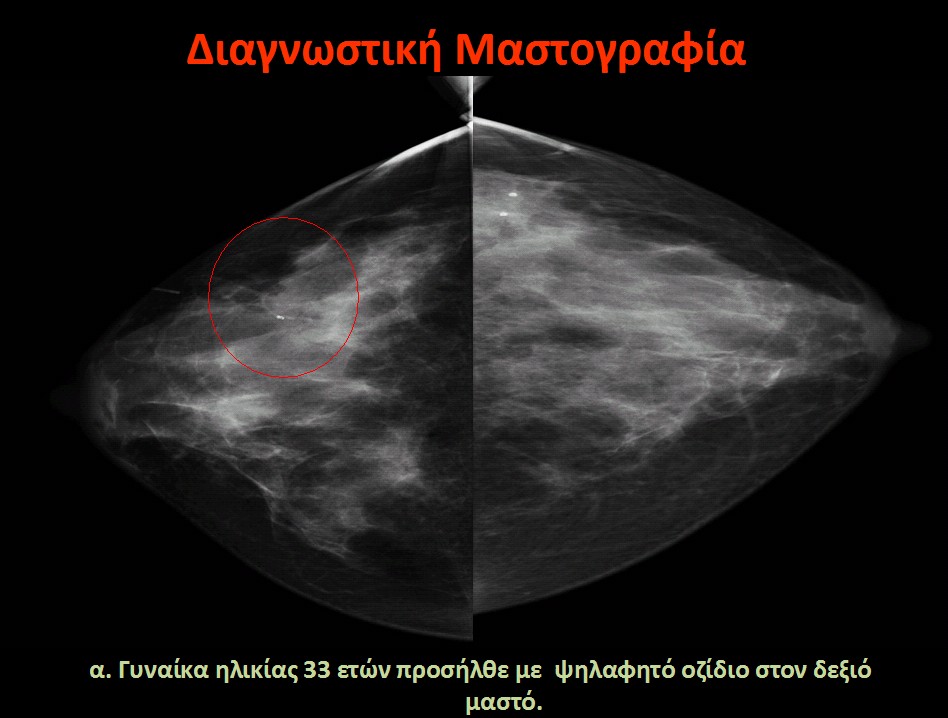
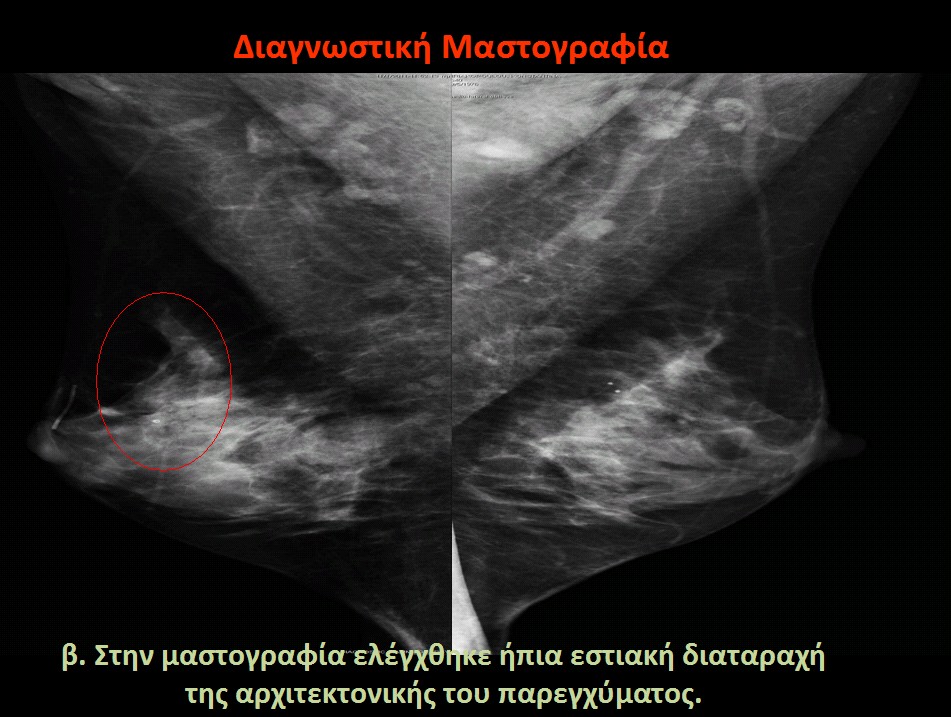
When a woman presents for a mammogram with a clinical finding found by her or by her clinician, the mammogram is called diagnostic. If the patient visits us with α palpable lump, an automatic nipple discharge or skin lesion, then further mammographic analysis is performed. This detailed analysis is conducted during the patient’s visit, immediately after the mammography to avoid the hassle of a second visit which extends the anguish and anxiety of the results.
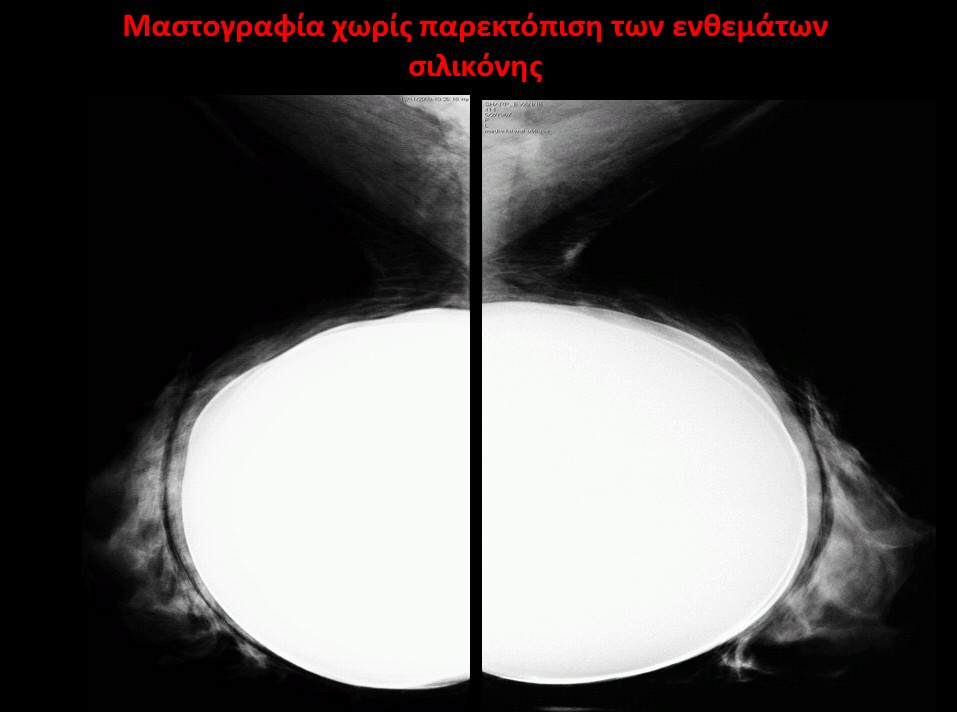
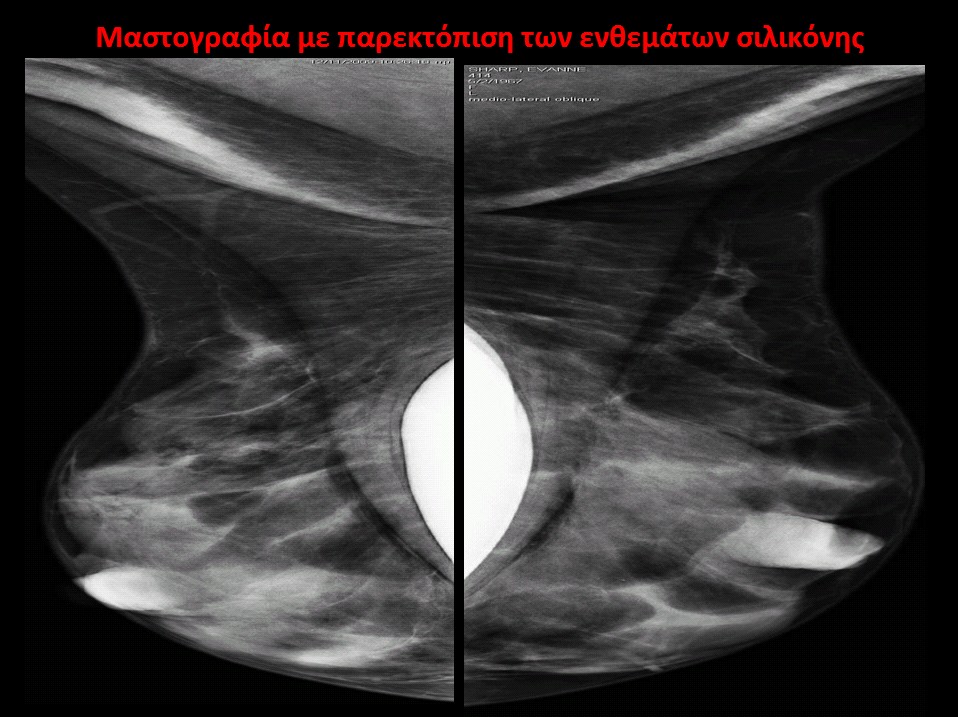
Mammography in women with silicone implants
Regardless of their size, silicone implants limit the diagnostic accuracy of mammography because they cover a large part of the breasts. At “Diagnostic Mammography”, we apply a special technique* to women with silicone implants, conducting the examination by taking special images with and without displacement **. This technique gives us the ability to examine the largest volume of the breasts; however, as it is written in the literature, about 20% of the total breast volume will still be covered by the implant, so it is impossible to evaluate the total breast tissue.
* Improved imaging of the augmented breast. Eklund GW, Busby RC, Miller SH, Job JS. AJR Am J Roentgenol. 1988 Sep;151(3):469-73. **When performing the mammography, we perform mild pressure on the silicone implants, pushing them towards the chest wall so as to reveal the largest possible part of the breast tissue in the mammographic field of view.
Mammography in small breasts
Women with small breasts present no problems to perform the examination. The experienced personnel of “Diagnostic Mammography” carefully places the breasts on the mammography unit and asks the woman to hold her breath for a few seconds in order to achieve successful images taken of the entire breast parenchyma.
Mammography after tumour excision and radiation
Operated breasts for tumour excision develop fluid collection and granulation tissue, which gradually minimize with time resulting in scarring, while after radiation breasts oedemas develop. Thus, while the mammography technique remains the same, the performance of the examination in these cases is more complicated and should be conducted by an experienced technologist. The tumour excision findings gradually subside after the first year, as progressive tissue repair is noted.
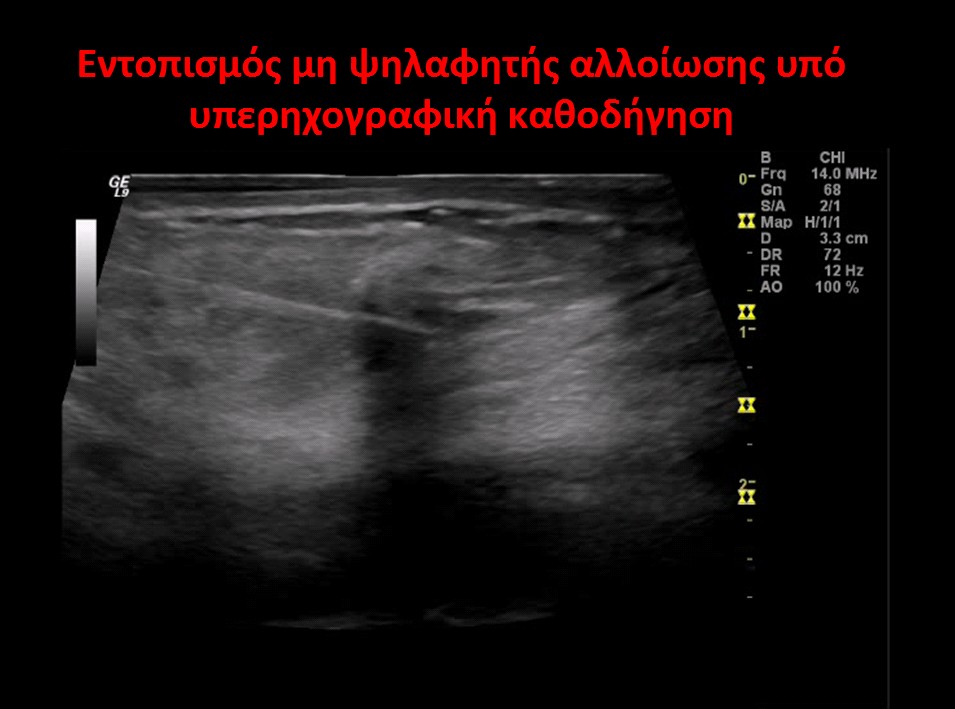
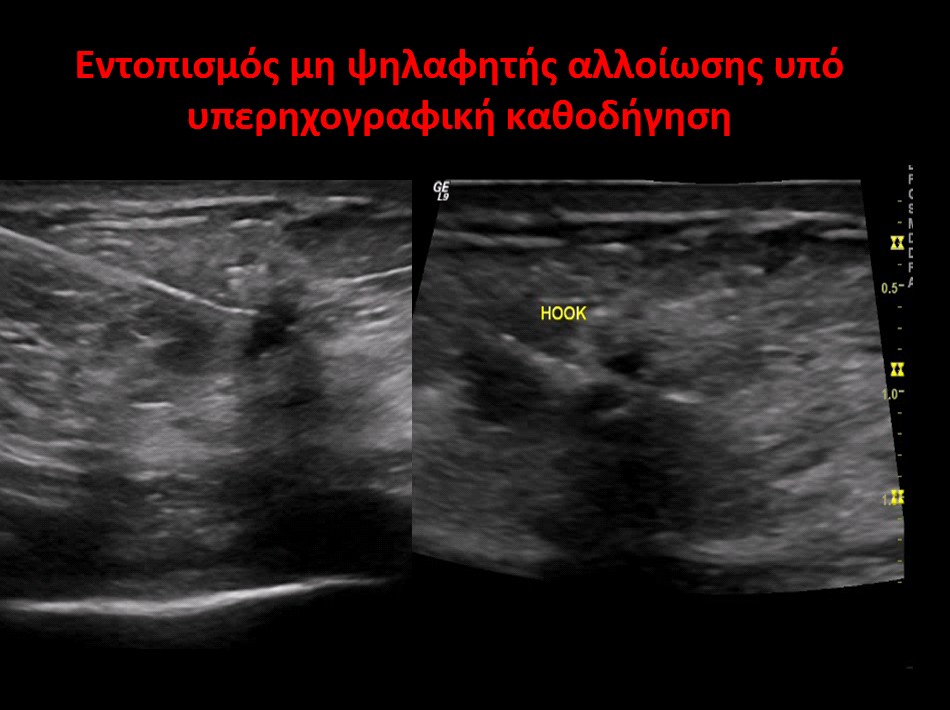
Detection of intangible lesions
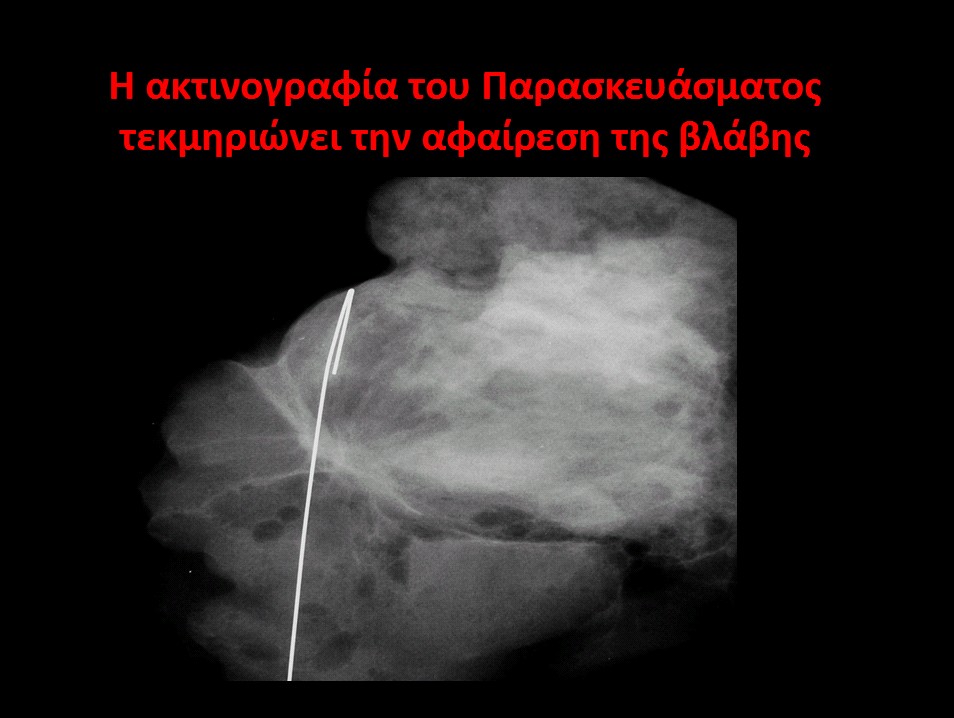
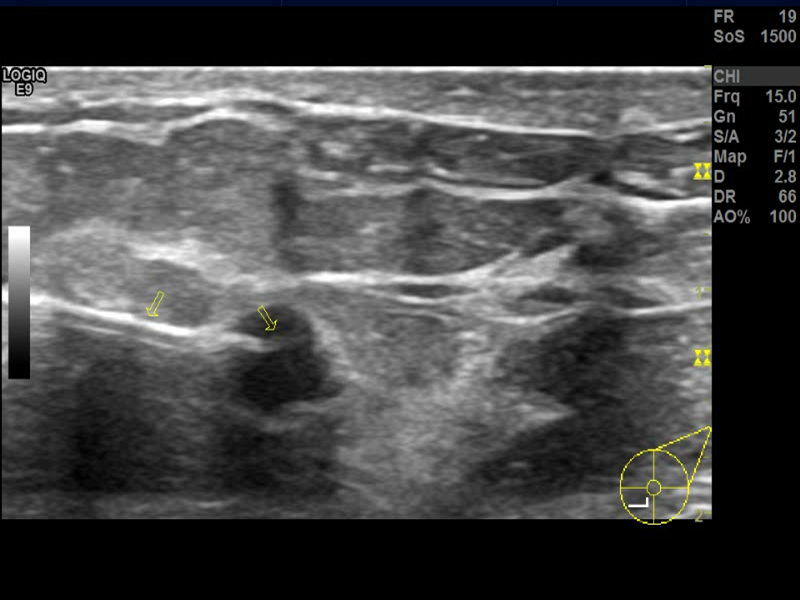
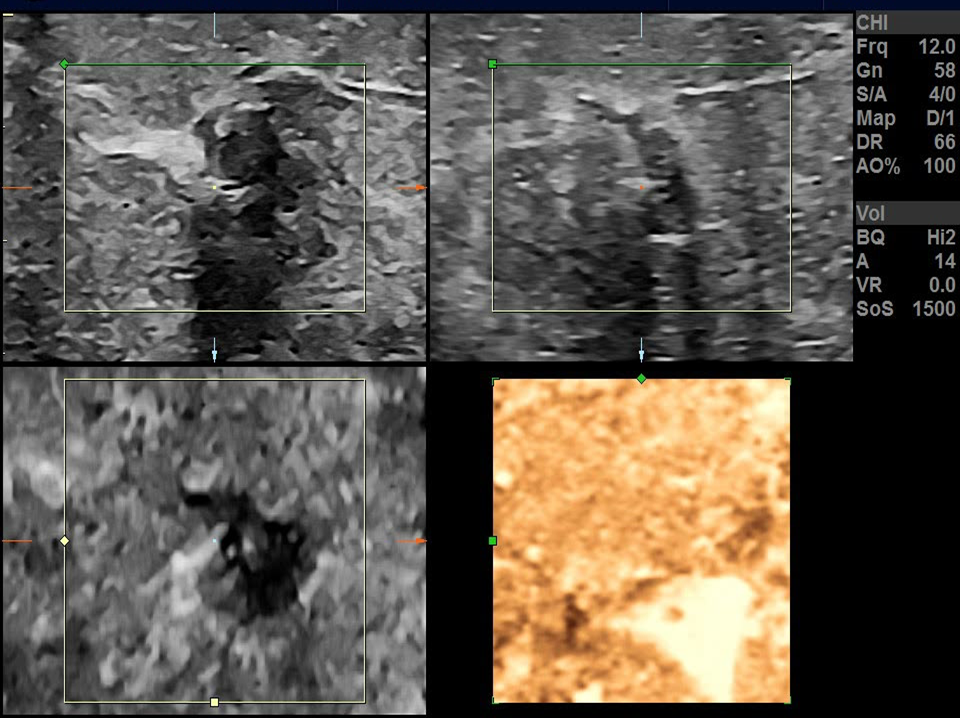
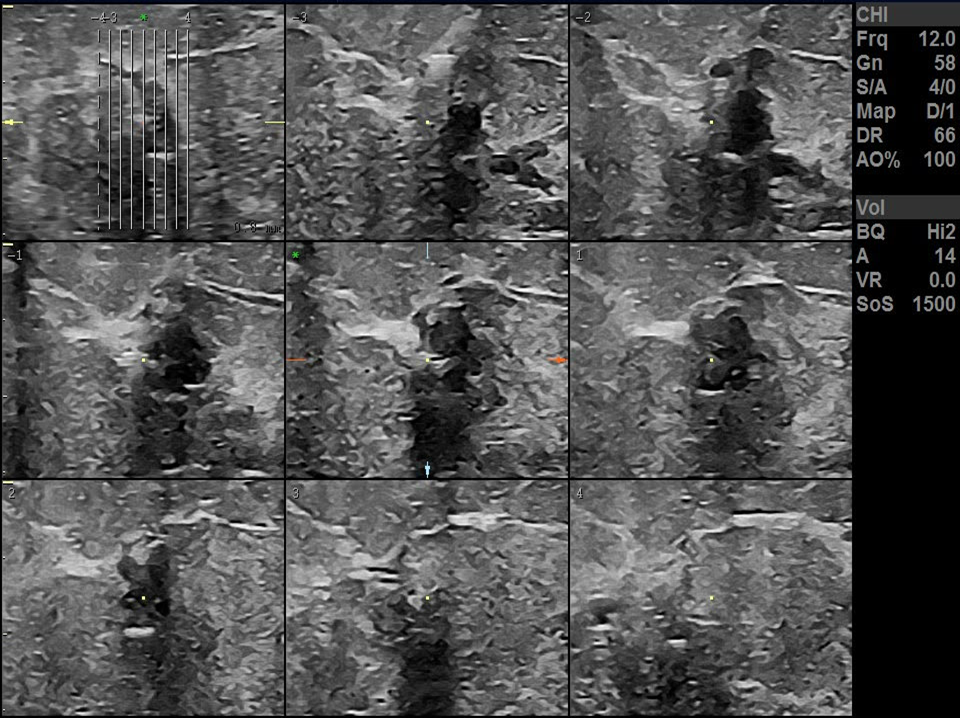
When an unexplained lesion is detected on a preventive mammogram or ultrasound, then the radiologist must proceed with the detection procedure. The “Diagnostic Mammography” center, for more than a decade, has been using the detection method. During this procedure, with the administration of a local anesthetic and the contribution of the mammogram or with the guidance of the ultrasound, the radiologist proceeds to the exact placement of the wire guide in the center of the lesion to remove it. The removed preparation is subjected to an x-ray or ultrasound to confirm that the lesion has been completely removed. According to the European Union guidelines, the radiologist is responsible for the detection process.
The mammography technique
Throughout the examination specialized assistance is given to women reassuring the correct position and posture until the end of the mammographic process.
The examination lasts about 5 minutes.
Women are asked to undress above the waist and put on a gown. The examinee stands in front of the machinery.
During the examination the assistant radiologist places each breast between two special plates receiving gentle pressure for a few seconds.
A total of four images are taken during the examination, two for each breast.
While each image is taken, the examinee should hold her breath for a few seconds in order to perceive maximum image sharpness.
The reliability of mammography
Physical and technical specifications of mammography
In order for mammography to be a reliable examination it should be technically perfect. The radiologist should be trained in the assessment of breast diseases correctly implementing examination study standards. According to literature an experienced radiologist who interprets a greater number of mammographies achieves a higher diagnostic accuracy.
Moreover, in accordance with EU guidelines, apart from specializing in breast diseases, radiologists are responsible for the excellent quality and technique of mammographies. Technologists (assistant radiologists), who must have specific knowledge regarding the technical aspects of mammography, are responsible for the proper functioning of the mammography units.
Criteria for the quality assessment of mammography
Under EU guidelines, the criteria for the quality assessment of mammographies are:
Proper placement of the breasts on the mammography unit to allow the inclusion of the entire breast, the sub mammary fold (fold below the breast), the axillary area and a part of the pectoral muscle on the mammography field.
The images must be symmetrical and very sharp.
The appropriate pressure must be performed to the breasts.
There should be no skin folds and the shoulders, lower jaw, hair, the abdomen or foreign objects such as jewellery, belts and other items should be excluded from the examination field.
Each breast should be properly included on the image and the examinee’s details should be correct.
Coding of results
For the better cooperation between radiologists and clinicians, which leads to a greater benefit for the patients, the results of mammograpies are coded. This coding started at the American College of Radiology (ACR), which introduced the Breast Imaging Reporting and Data System with the code (BI-RADS ®), being the result of collaboration of the ACR, the National Cancer Institute (NCA), the Center for Disease Control and Prevention, the Food and Drug Administration, the American Medical Association, the American College of Surgeons and the College of American Pathologists.
The results of each mammogram bear a code that depending on what is written is interpreted as:
BI-RADS 0: Assessment is incomplete. Further imaging examinations are needed.
BI-RADS 1: Negative mammogram.
BI-RADS 2: Benign findings.
BI-RADS 3: Probably benign findings, a deviation of 2% may concern lesions representing malignancy.
BI-RADS 4: Findings with a probability of malignancy (3-94%). Further investigation with a biopsy is necessary.
Category 4 is divided into 4a, 4b and 4c.
Category 4a includes lesions that have morphological characteristics that are suggestive of benign causes (degenerating fibroadenomas, complicated cysts).
Category 4b includes lesions that have a higher suspicion of malignancy. A histological examination is necessary.
Category 4c includes lesions that have morphological characters even more suspicious of malignancy. The lesion is further investigated with a biopsy.
BI-RADS 5: Findings with typical malignant characters. Further management is necessary.
BI-RADS 6: Malignant lesions confirmed by histological examination.
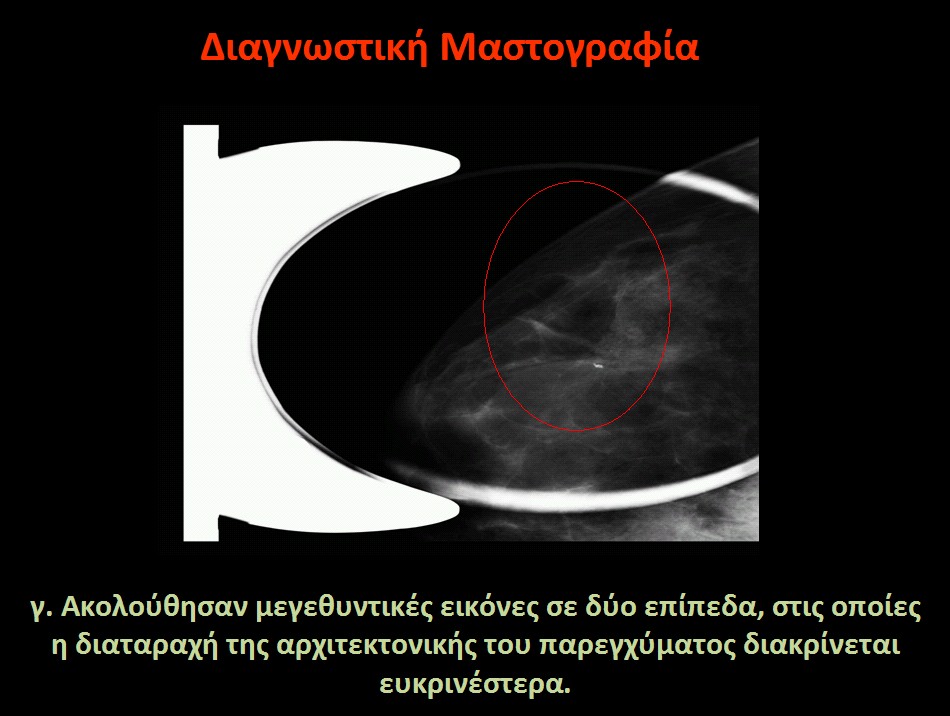
The special images taken
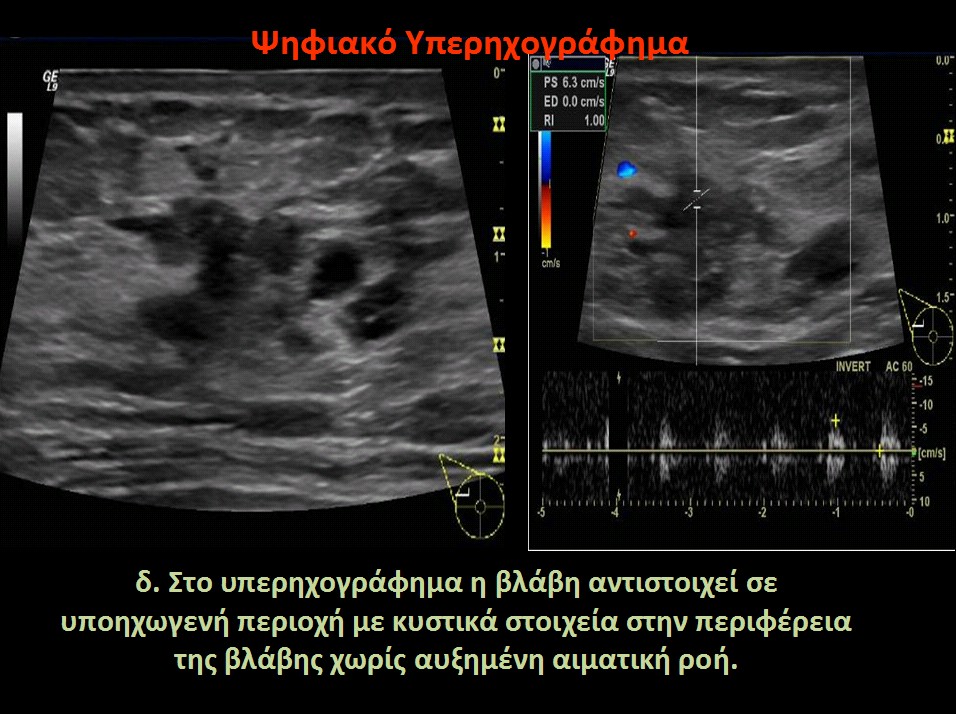
If a more thorough and detailed analysis of the breast is necessary, a further mammographic analysis is carried out by the technologist. In diagnostic solving cases an ultrasound is performed. The results of the images are interpreted by the radiologists and if the lesion remains suspicious, a further investigation with biopsy is indicated.
Management in the case of a negative mammogram and a positive clinical finding
There are cases where a woman presents with some clinical finding, such as palpable lump or palpable stiffness, but these findings are not detected on the mammography meaning that the examination results are interpreted as negative. Indeed, if this palpable finding is obscured on mammography due to high breast density but conceals a malignancy, then the consequences for the examinee can be hazardous. To avoid such devastating mistakes, a key requirement is to strictly follow the basic steps in the diagnostic approach and establish a close cooperation between the examinee and the team of experts who monitor the patient.
Specifically, all women should define the reason for their visit and should not rely only on the negative diagnosis of the mammogram. The radiologist should complete the imaging evaluation with an ultrasound and, regardless of the outcome of the examination, if there is a clinical finding, must refer the examinee to a clinician for further evaluation.










{kind=link}
{kind=link}
{kind=link}
{kind=link}